
Breaking the cycle
Dave Burnett
Breaking the cycle
It’s well established that chronic disease management for people with chronic obstructive pulmonary disease (COPD) has a positive impact on their lives. The concept of using a comprehensive care plan to treat chronic airway obstruction was first introduced by Thomas Petty, MD in 1969.[1] Providers have used a variety of strategies to provide chronic disease management to people with COPD including transitional care models, home health, community support services, pulmonary rehabilitation (PR), and most recently, technology. Personally, I’m very fond of and biased towards PR since I’ve spent 30 years witnessing the positive effects PR has on people with COPD and other chronic respiratory diseases.
Within our PR programmes we purposefully design tailored plans for our patients to optimize outcomes, so why not do the same for how people can access PR? If we leverage technology to complement and enhance traditional service delivery, can we support a more personalized way to access care?
To read the full article, simply fill out the form below.

T he Centers for Disease Control (CDC) report that 6.2% of the adults in the United States (US) have been diagnosed with chronic obstructive pulmonary disease (COPD)[1]. This accounts for nearly 16 million adults and over 146,000 deaths occur annually due to this preventable and treatable chronic condition.[2] Pulmonary rehabilitation (PR) has shown to have a positive impact on the lives of people with COPD. The concept of PR was first introduced by Petty et al in a 1969 publication titled, A comprehensive care program for chronic airway obstruction.[3] Over fifty years after this seminal article, a plethora of scientific evidence has shown that PR can optimize exercise capacity, improve dyspnea, enhance quality of life (QoL), and reduce costly hospital readmissions in people with COPD.[4] Moreover, a landmark study indicated that PR initiated within 90 days of discharge from the hospital for COPD lowers the risk of death by 37% within the first year.[5] Pulmonary rehabilitation is a vital treatment for patients with chronic respiratory disease, however there are significant gaps that limit its availability to those who could benefit the most. These gaps can be attributed to various factors, including geographical, socioeconomic and systemic challenges. In this article, Dr Dave Burnett explores how we can overcome these challenges to improve access to pulmonary rehabilitation, ensuring no patient is left behind. Sign up below to gain full access to this article and stay informed about our upcoming thought leadership series!
The my mhealth data library is an extensive resource designed to support healthcare providers by offering a wealth of information and tools related to COPD and long-term health conditions.
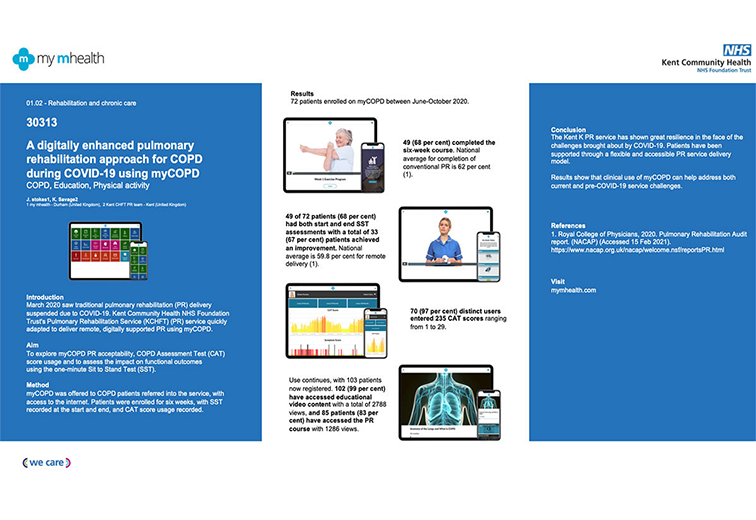
Results of a service evaluation by Southend University Hospital using myCOPD to support a home-based pulmonary rehabilitation (PR) programme in several different local locations. The Enhanced Pulmonary Rehabilitation Programme was launched by Southend University Hospital in 2018. The programme was designed to offer a variety of options for patients to complete their PR. This was a new model of care offered to patients who were unable to attend or were waiting for a centre-based course. This provided these patients with an opportunity to undertake an education and exercise course at home, supported by the PR team. The home-based PR programme recruited 88 patients to the evaluation. 59 of the 88 home-based PR patients chose to include myCOPD , of which 15 (17%) used myCOPD only and 44 (50%) used it in combination with written information and a DVD. The remaining 29 home-based patients did not wish to include myCOPD in their PR programme and were therefore provided with either written information or a DVD. Home-based completion rates showed that 31 (52.5 %) of the 59 patients using myCOPD at home completed the full PR programme in comparison to 7 (24.1%) of 29 who did not include the app. The COPD Assessment Test (CAT) was used as an outcome measure to explore the impact of the app for those at home. Results showed that all home-based groups saw an improvement in CAT score, however the greatest improvement overall was in the myCOPD alone group with a -3.7 point reduction. CAT score reduction across other groups ranged from -3.6 to -1.9. Despite small differences observed in CAT score between groups, there was a more than a 100% higher completion rate of the full PR programme in those using myCOPD compared to those who did not. The app has a structured PR programme for patients to follow at a time that suits them demonstrating the apps diverse capability. In-app notifications can be sent to remind patients to complete their PR programme and clinicians can monitor their progress. This evaluation supports the significant impact that the myCOPD app can provide to support patients and healthcare service delivery remotely and at scale across different locations. The evaluation also supports the findings from the much larger Trooper Study published in bmj.com.

Simon Bourne 1,2 Ruth DeVos 1,2 Malcolm North 2 Anoop Chauhan 1 Ben Green 1 Thomas Brown 1 Victoria Cornelius 3 Tom Wilkinson 2,4 Portsmouth Hospitals NHS Trust, Portsmouth, UK my mhealth Ltd Bournemouth, UK Imperial College, London, UK Clinical and Experimental Sciences, Faculty of Medicine, University of Southampton, Southampton, UK
Mal North 1 Simon Bourne 1 Ben Green 2 Anoop J. Chauhan 2 Tom Brown 2 Jonathan Winter 2 Tom Jones 2 Dan Neville 2 Alison Blythin 1 4, 5 Matthew Johnson 4 David Culliford 4 Jack Elkes 3 Victoria Cornelius 3 Tom M. A. Wilkinson 1, 2, 5 my mhealth Ltd Bournemouth, UK Portsmouth Hospitals NHS Trust, Portsmouth, UK Imperial College, London, UK NIHR ARC Wessex, University of Southampton, Southampton, UK Faculty of Medicine, University of Southampton, Southampton, UK First publication of complete results shows the myCOPD app could play an important role in supporting recovery following an exacerbation of COPD. The results from the RESCUE trial (MMH-R02), investigating the possible impact of myCOPD in supporting the recovery of patients admitted with an exacerbation of COPD were published in NPJ Digital Medicine Journal. Exacerbations of COPD are one of the commonest causes of admission and re-admission to hospital. The role of digital interventions to support self-management in improving outcomes is uncertain. We conducted an open, randomised controlled trial of myCOPD in 41 COPD patients recruited following hospital admission with an acute exacerbation. Subjects were randomised to either receive usual care, including a written self-management plan (n=21), or the myCOPD app (n=20) for 90 days. The primary efficacy outcome was recovery rate of symptoms measured by COPD Assessment Test (CAT) score. Exacerbations, readmission, inhaler technique quality of life and patient activation (PAM) scores were also captured. Results showed the app was acceptable in this care setting and was used by 17 of the 21 patients with sustained use over the study period. The treatment effect on CAT score was 4.49 (95% CI: -8.41, -0.58) points lower in the myCOPD arm. Patients’ inhaler technique improved in the digital intervention arm (101 improving to 20 critical errors) compared to usual care (100 to 72 errors). Exacerbations tended to be less frequent in the digital arm compared to usual care; 34 vs 18 events. Hospital re-admissions risk was 30 numerically lower in the digital intervention arm: OR for readmission 0.383 (95%CI 0.074, 1.987; 31 n=35). In this feasibility study of the digital self-management platform myCOPD, the app has proven acceptable. Its use has improved exacerbation recovery rates, with strong signals of lower re-exacerbation and re-admission rates over 90 days. myCOPD reduced the number of critical errors in inhaler technique compared to usual care with written self-management. This provides a strong basis for further exploration of the use of app interventions in the context of recently hospitalised patients with COPD.

Michael Crooks 1 Jack Elkes 2 William Storrar 3 Kay Roy 4 Mal North 5 Alison Blythin 5 Alastair Watson 6 Victoria Cornelius 2 Tom M.A. Wilkinson 5, 6 Hull York Medical School, Hull, UK Imperial College London, London, UK Hampshire Hospitals NHS Foundation Trust – Basingstoke Hospital, Basingstoke, UK West Hertfordshire Hospital NHS Trust – Hemel Hempstead Hospital, Hemel Hempstead, UK mymhealth Limited, Bournemouth, UK University of Southampton Faculty of Medicine, Southampton, UK First publication of complete results for a preliminary trial of a self-management intervention using a scalable app ( myCOPD) demonstrated signals of potential clinical benefit in a population of patients with mild-moderate and newly diagnosed COPD over a 90 day period. The results from the EARLY trial (MMH-R03), funded by an UKRI Innovate UK Grant to my mhealth were published in ersjournals.com. Self-management interventions in COPD aim to improve patients’ knowledge, skills and confidence to make correct decisions, leading to an improvement in health status and outcomes. myCOPD is a web-based self-management app known to improve inhaler use and exercise capacity in individuals with more severe COPD. We explored its impact in patients with mild-moderate or recently diagnosed COPD through a 12-week, open-label, parallel-group, randomised-controlled trial of myCOPD compared with usual care. The co-primary outcomes were between group differences in mean COPD assessment test (CAT) score at 90 days and critical inhaler errors. Key secondary outcomes were app usage and patient activation measurement (PAM) score. 60 patients were randomized overall (29 myCOPD, 31 usual care). Groups were balanced for FEV1% predicted, but baseline imbalance between groups for exacerbation frequency and CAT score. There was a trend to lower CAT scores in the myCOPD arm, but due to the size of the study there was no significant adjusted mean difference in CAT score at study completion, -1.27 (95% CI -4.47 to 1.92, p=0.44) lower in myCOPD. However, increasing app use was associated with greater CAT score improvement. The odds of ≥1 critical inhaler error was much lower in the myCOPD arm (adjusted odds ratio of 0.30 (0.09; 1.06, p=0.061)). The adjusted odds ratio for being in a higher PAM level at 90 days was 1.65 (0.46; 5.85) in favour of myCOPD. The small sample size and phenotypic difference between groups limited our ability to demonstrate statistically significant evidence of benefit beyond inhaler technique, this confirms the finding from previous studies that myCOPD can reduce inhaler technique errors by >70%. The findings of this study will now be used to power a much larger RCT to investigate the impact of myCOPD in this patient population.

O’Sullivan C 1 Stokes J 2 Blythin A 2 Dr. Kirk A 2 Dr. Ellison P 3 Marine and Oakridge Surgeries, South Coast Medical Group, Dorset my mhealth Limited, Bournemouth Dorset Intelligence & Insight Service, Our Dorset – Digital ‘Our Digital Dorset’ and ‘my mhealth’ conducted a study exploring the usage of myCOPD by tracking activity using the Dorset Intelligence and Insight Service (DiiS). Results showed positive uptake and usage with myCOPD, demonstrating improvement in CAT scores. Socioeconomic factors did not appear to negatively influence app activation. myCOPD supports the remote monitoring of patients with COPD. App activity and changes in CAT score were visible to clinicians through DiiS, contributing to a positive population health management approach.

Francis P Chmiel 1 MSc, DPhil; Dan K Burns 1 MSc, PhD; John Brian Pickering 1 DPhil; Alison Blythin 2 MRES; Thomas MA Wilkinson 2,3,4* PhD; Michael J Boniface 1* BEng School of Electronics and Computer Science, University of Southampton , Southampton , GB my mHealth Limited, Bournemouth , GB National Institute for Health Research Applied Research Collaboration Wessex, University of Southampton , Southampton , GB National Institute for Health Research Applied Research Collaboration Wessex, University of Southampton , Southampton , GB
R esearch MMH-R06 published in Published on Pub Med 24th October 2023 Christopher Duckworth 1 Michael J Boniface 1 Adam Kirk 2 Thomas M A Wilkinson 2 3 4 IT Innovation Centre, Digital Health and Biomedical Engineering, University of Southampton, Southampton, UK. my mHealth Limited, London, UK. National Institute for Health Research Applied Research Collaboration Wessex, University of Southampton , Southampton , GB Faculty of Medicine, University of Southampton, Southampton , GB



Contact Us
support@mymhealth.com